
Translate this page into:
Persistent sputum smear positivity among new cases of pulmonary tuberculosis after 2 months of self-administered outpatient treatment in Yaounde, Cameroon
*Corresponding author: Kuaban Alain, Chest Service, Jamot Hospital in Yaounde/Department of Internal Medicine and Specialties, Faculty of Medicine and Biomedical Sciences, The University of Yaounde I, Yaounde, Cameroon. kuabanallen@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Alain K, Nelly Gabrielle GB, Moses S, Christopher K. Persistent sputum smear positivity among new cases of pulmonary tuberculosis after 2 months of self-administered outpatient treatment in Yaounde, Cameroon. J Pan Afr Thorac Soc. 2024;5:115-21. doi: 10.25259/JPATS_7_2024
Abstract
Objectives:
The objective of this study was to determine the incidence of persistent sputum smear positivity (PSSP) and identify factors associated with it in new sputum smear-positive pulmonary tuberculosis (SSPPTB) patients after 2 months of self-administered outpatient treatment.
Materials and Methods:
This was a retrospective review of the records of a cohort of all consecutive new cases of SSPPTB followed up at the tuberculosis diagnostic and treatment center of the Jamot Hospital in Yaounde between January 2015 and December 2021. Multivariable logistic regression was used to relate baseline characteristics with PSSP at the end of the 2-month self-administered outpatient treatment.
Results:
A total of 3136 new cases of SSPPTB with a mean age of 35.88 ± 13.42 years, including 1866 (59.50%) males, were studied. Persistent positive sputum smears after 2 months of treatment were observed in 332 patients, giving a cumulative incidence of 10.59% (95% confidence interval [CI]: 9.51–11.66). Multiple logistic regression analysis showed that age ≥35 years (odds ratio [OR]: 1.51; 95% CI: 1.19–1.90; P = 0.001), male gender (OR: 1.38; 95% CI: 1.08–1.76; P = 0.010), and pre-treatment bacillary load in sputum smear ≥2+ (OR: 2.44; 95% CI: 1.81– 3.30; P = 0.001) were significantly and independently associated with PSSP.
Conclusion:
The rate of PSSP in new SSPPTB patients after 2 months of self-administered outpatient treatment is similar to rates observed before 2015. Direct observed therapy targeted at patients with factors associated with PSSP should be considered to improve outcomes.
Keywords
Tuberculosis
Treatment
Persistent smear positivity

INTRODUCTION
One of the important ways used to monitor the effectiveness of treatment in patients with sputum smear-positive pulmonary tuberculosis (SSPPTB) is to examine their sputum smears for acid-fast bacilli (AFB) at specific periods of their treatment. In new cases with SSPPTB, these examinations are carried out at the end of the 2-month intensive phase of treatment and the end of the 5th and 6th months of treatment.[1] The results of the follow-up examination of sputum smears at the end of the 2-month intensive phase are crucial, for it is known that persistent sputum positivity at the end of this phase of treatment predicts adverse outcomes in terms of treatment failure and relapse as well as default from treatment.[2-7] The persistence of sputum smear positivity at the end of this phase of treatment is all the more problematic from a public health perspective, as a significant proportion of these patients can still spread the disease.[8]
In Cameroon, before 2015 and in accordance with the guidelines of the National Tuberculosis Control Program (NTCP), all SSPPTB cases were systematically hospitalized during the intensive phase of treatment to ensure that they received directly observed therapy (DOT). The incidence of non-conversion of sputum smears in new cases of pulmonary tuberculosis (TB) at the end of the intensive phase of treatment at the TB diagnostic and treatment center (TBDTC) of the Jamot Hospital in Yaounde (JHY) was reported to be 13.4% and 10.2%, respectively, in 2009 and 2014.[9,10]
Since 2015 and in accordance with the new guidelines of the NTCP,[11] SSPPTB patients, except for severe and complicated cases, are no longer hospitalized but rather receive self-administered treatment on an outpatient basis throughout the entire treatment course. Since the treatment of patients is no longer administered under direct observation and supervision by the health personnel as was previously the case, the impact of this change in policy on the non-conversion of patients’ sputum smears at the end of the intensive phase of treatment is not known. This study aimed to determine the incidence of persistent positive sputum smears at the end of the 2-month intensive phase of anti-TB treatment in new cases of patients with SSPPTB and to identify some factors associated with it in the TB-DTC of the JHY.
MATERIALS AND METHODS
Study setting
The study was conducted at the TB-DTC of the Jamot Hospital in Yaounde (JHY), the main referral hospital for respiratory diseases in Yaounde and its surrounding areas. In this center, the diagnosis of SSPPTB is made on the basis of a suggestive clinical history and the presence of AFB on at least one of the sputum samples submitted for microscopic examination on 2 consecutive days after staining by the Ziehl–Neelsen’s technique. Cultures for mycobacteria are not done for suspected new cases of pulmonary TB.
All new SSPPTB cases, except for severe and complicated cases, are treated on an outpatient basis after benefiting from education on the modalities of treatment by the health staff of the TB-DTC. The total duration of treatment is 6 months. It consists of a 2-month intensive phase of daily rifampicin (R), isoniazid (H), ethambutol (E), and pyrazinamide (Z), followed by a 4-month continuation phase of daily rifampicin and isoniazid. Compliance to treatment during the intensive phase is assessed by weekly return for drug collection and during the continuation phase, by monthly return of the patients for drug refills.
During the 6-month treatment period, the patient’s sputum is checked thrice for the presence or absence of AFB by direct microscopic examination. This is done at the end of the 2-month intensive phase and the end of the 5th and 6th months of treatment. In patients whose sputum smears remain positive at the end of the intensive phase of treatment, an additional month of the intensive phase is given, followed by the continuation phase. The outcome of patients at the end of the 6 months of treatment is recorded into one of the following six mutually exclusive categories according to the recommendation of the International Union Against TB and lung disease[12] adopted by the NTCP:[11]
Cured: Treatment completed with a negative sputum smear in the past month of treatment and on at least one previous occasion.
Treatment completed: A patient who has completed treatment but does not meet the criteria to be classified as a cure or failure.
Treatment failure: A patient who is sputum smear-positive at 5 months or later during treatment.
Died: A patient who dies for any reason during treatment.
Lost to follow-up: Patient whose treatment is interrupted for 2 consecutive months or more.
Transferred out: A patient who has been transferred to another recording and reporting unit and for whom the treatment outcome is unknown.
Study design and population
The study was designed as a retrospective review of a cohort of all consecutive SSPPTB patients aged 15 years and above who were systematically put on treatment and followed up at the TB-DTC of the JHY between January 2015 and December 2021 (a total of 7 years). Patients who were transferred out to other TB centers who died or were lost to follow-up before the end of the intensive phase of treatment were excluded from the study.
Data collection
All consecutive new cases with SSPPTB who fulfilled the inclusion criteria over the study period were identified through a review of the TB register and the patients’ treatment forms. For each patient identified, the following information at baseline was extracted from the TB register and treatment form and recorded on a pre-prepared data collection form: Age (in years), sex, human immunodeficiency virus (HIV) infection status, and the sputum smear bacillary load at diagnosis graded semi-quantitatively (rare, 1+, 2+, and 3+). The result of the sputum smear bacillary load equally graded semi-quantitatively (negative, rare, 1+, 2+, and 3+) at the end of the intensive phase of treatment for each patient included was also extracted and recorded.
Data management and analysis
Data were double entered into a computer using the Epidata version 4.4.2.1 data entry software (Epidata Association, Odense, Denmark, http://www.epidata.dk). Discordances were identified and resolved through verification of the original paper record. Data analysis was performed using the IBM® SPSS (Statistical Package for the Social Sciences) version 28 software. The cumulative incidence of sputum smears non-conversion at the end of the 2-month intensive phase of anti-TB treatment was calculated as the proportion of study participants with a persistent positive sputum smear. Chi-square or, where appropriate, Fisher’s exact test was used to compare proportions. Multivariable logistic regression analysis was performed using variables found to be significantly associated or having borderline association (P < 0.1) with sputum smear non-conversion in the bivariate analysis to identify those that were independently associated with it. P < 0.05 was used to characterize significant results.
Ethical and administrative approval
The study received ethical approval from the Institutional Review Board of the Faculty of Health Sciences of the University of Bamenda (ID N0: 2022/0418H/UBa/IRB). Administrative authorization to conduct the study in the TBDTC of the JHY was obtained from the hospital administration (ID N0: 00000573/L/MINSANTE/SG/DHJ). Patient consent for this study was waived because this was a study with data collected de-identified. The research methods used in this article are in full compliance with the Helsinki Declaration.
RESULTS
During the study period, a total of 4042 new patients with SSPPTB were enrolled in treatment at the TB-DTC of the JHY. Of these 4042 patients, 906 were excluded from the study. Figure 1 presents the flow chart showing the selection of patients retained for the study. There was, however, no statistical difference with respect to age and sex between those excluded and the 3136 patients aged 15 years and above who were retained for the analysis.
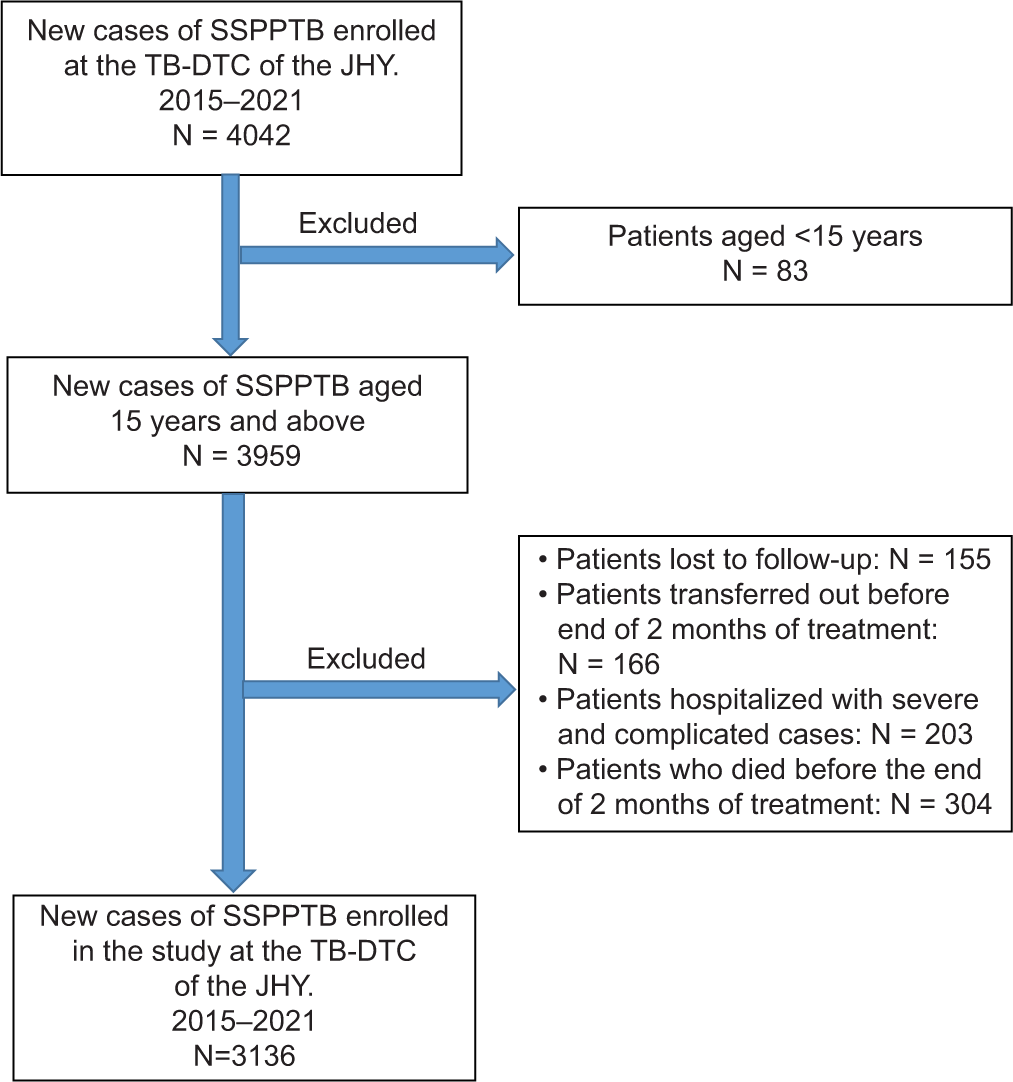
- Flow chart showing the selection of study participants. JHY: Jamot Hospital in Yaounde, SSPPTB: Sputum smear-positive pulmonary tuberculosis, TB-DTC: Tuberculosis diagnostic and treatment center.
General characteristics of the study population
Of the 3136 patients included in the study, there were 1866 (59.50%) males and 1270 (40.50%) females, with a mean age of 35.88 ± 13.42 years (range 15-93 years). Out of the 3136 included, HIV status was known for 3047 (97.2%) patients and 828 (27.17%) were HIV positive. The majority (68.97%) of the patients had a pre-treatment bacillary load on sputum smears of 2+ or more [Table 1].
| Characteristic | Number (n=3136) | Percentage (%) |
|---|---|---|
| Age | ||
| Mean age (SD) years | 35.88 (13.42) | |
| <35 years | 1663 | 53.03 |
| ≥35 years | 1473 | 46.97 |
| Sex | ||
| Male | 1866 | 59.50 |
| Female | 1270 | 40.50 |
| HIV status | ||
| Positive | 828 | 26.40 |
| Negative | 2219 | 70.76 |
| Unknown | 89 | 2.84 |
| Pre-treatment bacillary load | ||
| +1 | 973 | 31.03 |
| +2 | 1201 | 38.30 |
| +3 | 962 | 30.67 |
HIV: Human immunodeficiency virus, SD: Standard deviation
Incidence of persistent sputum smear positivity at the end of the 2-month intensive phase of treatment
Table 2 presents the distribution of patients according to their sputum smear results at the end of the 2-month intensive phase of anti-TB treatment. Three hundred and thirty-two of the 3136 patients studied were still sputum smear-positive, giving a cumulative incidence of persistent positive sputum smears of 10.59% (95% confidence interval [CI] = 9.51–11.66).
| Sputum smear results at the end of the intensive phase | Number (n=3136) | Percentage (%) |
|---|---|---|
| Negative | 2804 | 89.41 |
| 1+ | 272 | 8.67 |
| 2+ | 54 | 1.72 |
| 3+ | 6 | 0.19 |
Factors associated with persistent positive sputum smears at the end of the intensive phase of treatment
The characteristics of patients with and without persistent positive sputum smears at the end of the 2-month intensive phase of anti-TB treatment are summarized and compared in Table 3. Bivariate analysis revealed that sputum smear non-conversion was associated with an age ≥35 years (P = 0.001), the male sex (P = 0.001), and having a pre-treatment bacillary load in sputum of 2+ or more (P = 0.001). On the multivariable level, including only these factors that were associated with persistent smear positivity in bivariate analysis, age ≥35 years (odds ratio [OR]: 1.51; 95% CI: 1.19–1.9; P = 0.001), the male sex (OR: 1.38; 95% CI: 1.08–1.76; P = 0.010), and pre-treatment bacillary load of 2+ or more (OR: 2.44; 95% CI: 1.81–3.30; P = 0.001) remained as significant independent factors associated with persistent positive sputum smears at the end of the intensive phase of anti-TB treatment of new cases with pre-treatment positive sputum smears [Table 4].
| Characteristic | Sputum smear positive (n=332) | Sputum smear negative (n=2804) | P-value |
|---|---|---|---|
| Age, n (%) | |||
| ≥35 years | 187 (56.33) | 1286 (45.86) | <0.001 |
| <35 years | 145 (43.67) | 1518 (54.14) | |
| Gender, n(%) | |||
| Male | 225 (67.77) | 1641 (58.52) | 0.010 |
| Female | 107 (32.23) | 1163 (41.48) | |
| HIV status, n(%) | |||
| Positive | 82 (25.39) | 746 (27.39) | 0.445 |
| Negative | 241 (74.61) | 1978 (72.61) | |
| Pre-treatment bacillary load, n(%) | |||
| ≥2+ | 277 (83.43) | 1886 (67.26) | <0.001 |
| <2+ | 55 (16.57) | 918 (32.74) |
HIV: Human immunodeficiency virus
| Variable | B-coefficient | P-value | OR | 95% CI |
|---|---|---|---|---|
| Age ≥35 years | 0.408 | <0.001 | 1.51 | 1.19–1.90 |
| Male sex | 0.320 | 0.010 | 1.38 | 1.08–1.76 |
| Pre-treatment bacillary load ≥2+ | 0.892 | <0.001 | 2.44 | 1.81–3.30 |
OR: Odds ratio, CI: Confidence interval
DISCUSSION
Sputum smear microscopy continues to be the main tool used in most low-income countries for monitoring the effectiveness of treatment in patients diagnosed with sputum smear-positive pulmonary TB despite the controversies surrounding its usefulness. Several studies have shown, however, that persistent positive sputum smears at the end of the 2-month intensive phase of anti-TB treatment in new cases of smear-positive pulmonary TB are one of the strongest predictors of treatment failure.[2-5] Meanwhile, the controversy raised by the persistence of sputum smear positivity at the end of the 2-month intensive phase of treatment arises from the fact that the predictive value of a smear result at the end of the 2nd month is rather high when the result is negative but considerably less so when it is positive.[13] Indeed, a positive sputum smear for AFB does not permit one to know whether these are still viable bacilli or not after 2 months of anti-TB treatment. To assess sputum sterilization correctly, it is ideal to study sputum cultures for mycobacterial growth at the end of 2 months of treatment, as microscopy may also show non-viable or dead bacilli. Under program conditions, however, particularly in most low-income countries like Cameroon, cultures for mycobacteria are not usually available under field conditions. Meanwhile, the possible role of a smear-positive status by the end of the 2nd month of treatment can presently be used as a surrogate to warrant the susceptibility testing of sputum specimens of these patients for at least rifampicin resistance given the availability now of the Xpert Mycobacterium tuberculosis/Rifampicin (MTB/RIF) assay (Cepheid GeneXpert® System, USA), which not only detects MTB in specimens but also its resistance to rifampicin, a surrogate marker for multidrug-resistant TB.
The incidence of persistent sputum smear positivity (PSSP) in new cases of smear-positive pulmonary TB in this study was 10.59%. This is lower than the rate of 13.4% reported by Kuaban et al.[9] but almost similar to the rate of 10.2% reported by Pefura-Yone et al.[10] in similar studies in the same TB-DTC of the JHY, respectively, in 2009 and 2014. The result of this study suggests, therefore, that the magnitude of sputum smear non-conversion has remained stable and has not been affected negatively by the abolition of the policy of hospitalization of patients during the intensive phase of treatment meant to ensure that the health personnel directly observed the treatment of patients. This stability of the incidence of sputum smear non-conversion can probably be explained by the health education given to the patients with insistence on adherence to treatment as prescribed by the health staff of the DTC of the hospital at the start of their treatment and during their weekly return for their drug refill.
In this study, we assessed some factors in new cases with sputum smear-positive pulmonary TB in a bid to identify those that could be associated with persistent positive sputum smears at the end of the 2-month intensive phase of treatment. Bivariate analysis of these factors showed that an HIV seropositive status was not significantly associated with non-conversion of positive sputum smears. Of the factors that showed a significant association with PSSP at the end of the 2-month intensive phase of anti-TB therapy on bivariate analysis, age ≥35 years, the male sex, and a pre-treatment sputum smear bacillary load ≥2+ remained as independent significant factors of non-conversion of sputum smears on multivariable analysis.
HIV-positive status was not associated with the persistence of positive smears at the end of the 2-month intensive phase of treatment in our study. Our results are in agreement with those of several studies that have shown that there is no association between HIV status and delay in bacteriological conversion.[9,14-16] However, several factors exist that could potentially cause patients with an HIV-positive status to have delayed bacteriological conversion of sputum smears. Firstly, it has been reported that TB and HIV coinfection enhances the risk of harboring and acquiring drug-resistant strains, particularly in high TB burden settings,[17] a situation that can lead to delayed conversion of sputum smears. Second, adherence to treatment is a major challenge for this group of patients, given the higher pill burden that they must take, overlapping or additive adverse reactions, and drug-to-drug interactions[17,18] that may expose this group of patients to a delay in the bacteriological conversion of sputum smears. In addition, some biological mechanisms have been reported to contribute to drug resistance in HIV-infected individuals, and impaired drug absorption is one of the reasons for the ineffectiveness of TB treatment in this group of patients, particularly with such drugs as rifampicin and ethambutol.[19,20]
In this study, age ≥35 years was an independent predictor of persistent positive sputum smears at the end of the 2-month intensive phase of treatment. Our results are similar to those reported by several authors[6,9,21] who observed that age ≥40 years is associated with PSSP at the end of the intensive phase of treatment. The precise reason for this association is not known. However, this could probably be explained by the fact that patients at this age, due to socioeconomic challenges, such as losing hours from their jobs to attend health facilities for treatment, may not adhere properly to the taking of their medications.[22] In addition, age-related impairment of the immune system in these patients may lead to poor clearance of mycobacteria from the lungs.[21]
Men were less likely than women in this study to have sputum smears converted at the end of the 2-month intensive phase of treatment. Our result is in line with the findings reported by other authors.[4,23,24] This finding probably reflects the behavioral differences between men and women with respect to the taking of medications. Indeed, male patients have been reported to have treatment failure due to irregular taking of medicines as compared to women.[23] Our result, however, differs from those of a similar study carried out in the same TB-DTC of the JHY in 2009, in which no difference between the two sexes with respect to sputum smear non-conversion was observed.[9] This may be explained by the fact that at that period, patients were all hospitalized during the intensive phase of treatment, with medications being administered under direct observation and supervision by the health personnel.
In this study, a pre-treatment bacillary load in sputum smears of ≥2+ was also an independent predictor of persistent positive sputum smears at the end of the intensive phase of treatment. Many authors have reported on the influence a pre-treatment bacillary load has on sputum smear conversion at the end of the intensive phase of treatment.[4,6,9,14,15] For example, Singla et al.[6] reported that patients with numerous bacilli on pre-treatment sputum smears had an almost six-fold greater risk of sputum smear non-conversion than patients with few bacilli. Meanwhile, in a study from the Gambia, Lienhardt et al.[4] observed that sputum smear conversion at the end of the intensive phase of treatment in patients with sputum smear of 1+, 2+, and 3+ was 96.2%, 85.3%, and 81.8%, respectively. Our result agrees with the findings of these authors. PSSP in patients with a pre-treatment bacillary load in sputum smears of ≥2+ could be due to a clinical failure because of poor adherence to anti-TB treatment. This will suggest the need for DOT under the supervision of health personnel targeting such patients. It could also possibly arise from the resistance of their TB disease to anti-TB drugs. This will support the notion that patients with a pre-treatment bacillary load of 2+ or more may constitute a high-risk group for drug resistance, especially multidrug or rifampicin resistance (MDR/RR). As such, this group of patients could be included in the high-risk group of patients for MDR/RR-TB so that they could benefit from drug susceptibility testing. A rapid molecular test such as MTB/RIF (Cepheid Sunnyvale CA, USA), which not only detects MTB in sputum but also its resistance to rifampicin, could be adopted for this purpose. Patient’s consent not required as patients identity is not disclosed or compromised. Cost-effectiveness studies may, however, be needed to judge the appropriateness of this strategy in resource-limited settings such as Cameroon.
Our study was limited by its retrospective design and the operational nature of the study, which relied solely on information routinely collected and maintained in the TBDTC of the JHY. As such, we were unable to assess some other potential risk factors for sputum smear non-conversion at the end of the 2-month intensive phase of treatment in our study population. We, however, think that the retrospective nature of our study is likely to have only a minimal impact on our results because the regular supervision and monitoring activities of the center by the NTCP are quite robust. Second, as the study was conducted only in one of the DTCs of Cameroon, our results may not be easily generalized to all the new SSPPTB patients treated in other centers of the country. This notwithstanding, the strength of our study lies in the large sample size of the patients studied, with a relatively large number of patients with persistent positive sputum smears at the end of their intensive phase of treatment.
CONCLUSION
The rate of PSSP in new SSPPTB patients after 2 months of self-administered outpatient treatment is similar to rates observed before 2015. Age ≥35 years, the male gender, and a pre-treatment sputum smear bacillary load ≥2+ were the most significant factors associated with PSSP. It is, therefore, recommended that patients with these features be given the 2-month intensive phase treatment under direct observation and supervision by health personnel. In addition, patients who, despite this measure, remain sputum smear positive should benefit from an Xpert MTB/RIF assay to determine if their disease is rifampicin-resistant or not and be treated accordingly if this is the case.
Acknowledgments
We sincerely thank all the staff of the TB diagnostic and treatment center who provided us with their TB registers and patient treatment forms for review.
Ethical approval
The research/study was approved by the Institutional Review Board at Institutional Review Board of the Faculty of Health Sciences of the University of Bamenda, number ID N0: 2022/0418H/UBa/IRB, dated 21st May 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- National Tuberculosis Control Programme: Manual for health personnel Yaounde: Cameroon Ministry of Public Health; 2002.
- [Google Scholar]
- Sputum smear conversion during directly observed treatment for tuberculosis. Tuber Lung Dis. 1996;77:124-9.
- [CrossRef] [PubMed] [Google Scholar]
- Sputum microscopy results at two and three months predict outcome of tuberculosis treatment. Int J Tuberc Lung Dis. 1997;1:570-2.
- [Google Scholar]
- Factors determining the outcome of treatment of adult smear-positive tuberculosis cases in The Gambia. Int J Tuberc Lung Dis. 1998;2:712-8.
- [Google Scholar]
- Sputum smear status at two months and subsequent treatment outcome in new patients with smear-positive pulmonary tuberculosis. Int J Tuberc Lung Dis. 1999;3:1047-8.
- [Google Scholar]
- Factors predicting persistent sputum smear positivity among pulmonary tuberculosis patients 2 months after treatment. Int J Tuberc Lung Dis. 2003;7:58-64.
- [Google Scholar]
- Identifying early treatment failure on category I therapy for pulmonary tuberculosis in Lima Ciudad, Peru. Int J Tuberc Lung Dis. 2004;8:52-8.
- [Google Scholar]
- Prolonged infectiousness of tuberculosis patients in a directly observed therapy short-course program with standardized therapy. Clin Infect Dis. 2010;51:371-8.
- [CrossRef] [PubMed] [Google Scholar]
- Non conversion of sputum smears in new smear positive pulmonary tuberculosis patients in Yaoundé, Cameroon. East Afr Med J. 2009;86:219-25.
- [CrossRef] [PubMed] [Google Scholar]
- Non-conversion of sputum culture among patients with smear positive pulmonary tuberculosis in Cameroon: A prospective cohort study. BMC Infect Dis. 2014;14:138.
- [CrossRef] [PubMed] [Google Scholar]
- National tuberculosis control programme: Manual for health personnel Yaounde: Cameroon Ministry of Public Health; 2015.
- [Google Scholar]
- Management of tuberculosis: A guide to the essentials of good practice Paris, France: International Union against Tuberculosis and Lung Disease; 2010.
- [Google Scholar]
- Appropriateness of extending the intensive phase of treatment based on smear results. Int J Tuberc Lung Dis. 2004;8:114-6.
- [Google Scholar]
- Tuberculosis chemotherapy and sputum conversion among HIV-seropositive and HIVseronegative patients in South-Eastern Uganda. East Afr Med J. 1999;76:307-13.
- [Google Scholar]
- Factors influencing time to sputum conversion among patients with smear-positive pulmonary tuberculosis. Clin Infect Dis. 1997;25:666-70.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of sputum culture conversion among patients with tuberculosis in the era of tuberculosis resurgence. Arch Intern Med. 1999;159:1110-6.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-resistant tuberculosis and HIV infection: Current perspectives. HIV AIDS (Auckl). 2020;12:9-31.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of tuberculosis and the drug interactions associated with HIV-TB Co-infection treatment. Front Trop Dis. 2022;3:834013.
- [CrossRef] [Google Scholar]
- Association between HIV/AIDS and multi-drug resistance tuberculosis: A systematic review and meta-analysis. PLoS One. 2014;9:e82235.
- [CrossRef] [PubMed] [Google Scholar]
- Malabsorption syndromes in patients with tuberculosis as a cause of ineffective treatment: How to diagnose and overcome? Infus Chemother. 2020;3:24-5.
- [CrossRef] [Google Scholar]
- Predictors of time to sputum smear conversion in patients with pulmonary tuberculosis under treatment. New Microbiol. 2019;42:171-5.
- [Google Scholar]
- Predictors of outpatient medical appointment attendance among persons with HIV. AIDS Care. 1999;11:361-73.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors of delayed sputum conversion among patients treated for smear positive PTB in Northwestern rural Tanzania: A retrospective cohort study. Trop Med. 2017;2017:5352906.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of delayed sputum smear and culture conversion among a Portuguese population with pulmonary tuberculosis. Rev Port Pneumol. 2012;18:72-9.
- [CrossRef] [PubMed] [Google Scholar]




